



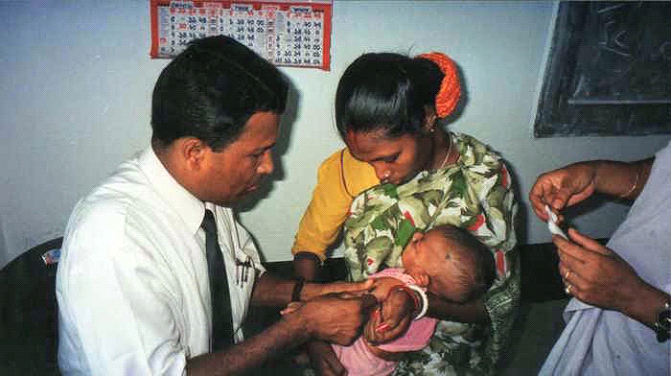
Sometime in 1989, Dr. Brahmochary was ready to receive the poor mother and child in his humble health centre, which was in Sonarpur, then a remote village. The groundwork was satisfactory. The dilapidated building's room, in which he was now sitting, was ready, though it smelt bit musty, after all it had been a cowshed. The scrubs in the surrounding were cleared, he could now see the road running along the front ground. His physician friends in the city remained standby to whom he would refer severe cases, and from them he would also get the donation of medicines and money. He had the consent of the local leaders, mostly the male family-heads, that their female family members and children were allowed to come to the centre. He was content to think that he would be able to save resource and time of the sick mothers and children from going to the city for their treatment.

Severe malnutrition Dr. Brahmochary had no mistake to understand that hunger lives as malnutrition among the mother and child. Perpetual hunger plants malnutrition in body, by diminishing its resistance, and once body resistance is gone, illness nestles in the body. Then the illness attacks the feeble malnutrition, and when malnutrition gives in, the total damage of the body takes place bringing complete death of a poor body. In medical science most commonly known malnutrition is Protein Energy Malnutrition (PEM). It can be discovered when a poor family continuously lacks protein as well as calories in their inadequate food of low quantity and quality, which is not uncommon in the West Bengal's rural areas. The modern medical science says that when a poor man lacks calories, his body consumes existing protein to make body-fuel, and thus calories fail to rebuild necessary tissues to build up healthy body. There are two types of PEM: Kwashiorkor and Marasmus. Kwashiorkor creates an invisibly acute situation in a body, which we normally fail to notice looking at the sufferer. It basically damages the tissue inside body and covers it with water. We may see a child in his mother's lap with round face and swollen cheeks, unusually quiet, without any zest. In reality, the Kwashiorkor has made him miserable, withdrawn and inactive. On the other hand, Marasmus is sadly visible as it makes the victim too thin, pushing him to go down to 40 per cent less than normal weight, and his situation often attracts the attention of media. Poor diet for a long period stops his normal growth, and the body consumes all of his tissues. A child of Marasmus looks like shrunken mature man with broad head, thin hair, sunken eyes, loose fat-less skin, and mostly he is unable to move on his own while certain death looms behind him. Not only in children, Dr. Brahmochary also found PEM in women. PEM nestles in women as anaemia, lacking sufficient red cells in blood, making them lethargic, fatigue, indifference, eliminating mental and physical capacities. He was more concerned that the presence of PEM in pregnant mother. The reason is that PEM affected mother carries PEM affected foetus that brings a malnourished, unhealthy child in the ever challenging world.
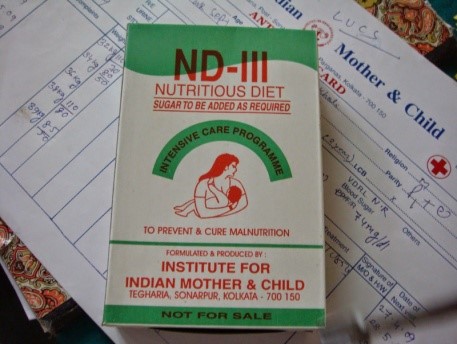
Simple nutritious food Dr. Brahmochary thought it was imperative first to strike the deadly interplay of hunger and malnutrition among poor mothers and children. He could foresee that without dealing with this chronic problem it would be difficult for them to change the poverty-laden societies. At the nascent stage of IIMC, he understood that dealing with malnutrition and hunger should be a recurrent activity as the prevailing socio-economic situation unable to assure the poor people with adequate healthy food. Presently, IIMC strongly advocates for nutritious food for poor rural mothers and children. Dr. Brahmochary has set an example of making a popular nutritious food in combination of locally available grains, which is cheap in price, easy to buy for poor family. To deal with the malnutrition at three stages, they are named as ND-S, ND-1 and ND-III, and the formula for the combination is available at IIMC. Besides, there is an arrangement of cooking and feeding this nutritious food for the ill mothers and children who are admitted to IIMC hospitals, and the message about this food goes to IIMC's working areas along with health education campaign. Once the mother and child gain their health, IIMC encourages them to adopt the challenge for building healthy life through education and income generation. According to Dr. Brahmochary, healthy mother and child are the strong pioneers for achieving empowerment.